Why an Athlete's Blood Sugar Plays by Different Rules
Understanding Physiologic Insulin Resistance
If you're a dedicated athlete — especially one logging long hours of aerobic training — you may have noticed something strange the morning after a big session: a fasting glucose reading that runs a little high, or a sluggish response on a glucose tolerance test, even though you're lean, fit, and by every other measure metabolically healthy. It can be unsettling if you don't know what you're looking at. But this pattern has a name, a well-documented mechanism, and a large body of exercise physiology research behind it: physiologic insulin resistance, also called glucose sparing.
As a highly trained endurance athlete, this response may be amplified. It is a normal metabolic adaptation in which the muscles temporarily rely more on fat for fuel while preserving glucose for the tissues that depend on it most — chiefly the brain and central nervous system. Unlike the insulin resistance seen in type 2 diabetes, this adaptation occurs despite excellent metabolic health, and it is generally considered a beneficial, rather than harmful, consequence of long-term endurance training.
The Biochemistry Behind the Adaptation
The root of glucose sparing traces back to a mechanism first described more than sixty years ago: the glucose–fatty acid cycle, also known as the Randle cycle. Randle and colleagues showed that when fatty acid availability and oxidation rise in muscle, byproducts of fat metabolism inhibit the enzymes responsible for glucose uptake and oxidation, effectively shifting the cell's fuel preference toward fat and away from glucose[1]. In an endurance-trained muscle, this isn't a malfunction — it's a finely tuned dial. Years of aerobic training increase the number and efficiency of mitochondria and the enzymatic machinery for burning fat, so trained muscle can lean on fat oxidation more readily and more efficiently than untrained muscle[7].
This is where the well-known “athlete's paradox” comes in. Research on endurance athletes has repeatedly found that they store more fat inside their muscle fibers (intramyocellular lipid) than sedentary or even obese individuals — a trait that, in a sedentary person, would predict insulin resistance and poor metabolic health. Yet endurance athletes remain highly insulin-sensitive overall[2]. The explanation lies in oxidative capacity and lipid quality: trained muscle has the mitochondrial machinery to actually burn the fat it stores, and the specific lipid species that accumulate (certain diacylglycerols, in particular saturated/unsaturated combinations) appear metabolically neutral or even favorable, unlike the lipid signatures associated with sedentary insulin resistance[3,4]. In other words, having more fuel available in the “tank” isn't the problem; what matters is whether the engine is built to use it, and an endurance athlete's engine is.
Glucose Sparing in Real Time
This adaptation isn't just a lab curiosity — it shows up directly in how trained athletes respond to prolonged exercise and in continuous glucose monitor (CGM) data. One 2023 study found that after three hours of continuous, moderate-intensity cycling, endurance athletes showed measurably reduced glucose tolerance and lower insulin sensitivity the following day, alongside elevated free fatty acids and ketones and a heightened reliance on fat oxidation[5]. Interval-style training did not produce the same effect, suggesting that it's specifically the prolonged, glycogen-depleting effort that triggers this temporary fuel-partitioning shift.
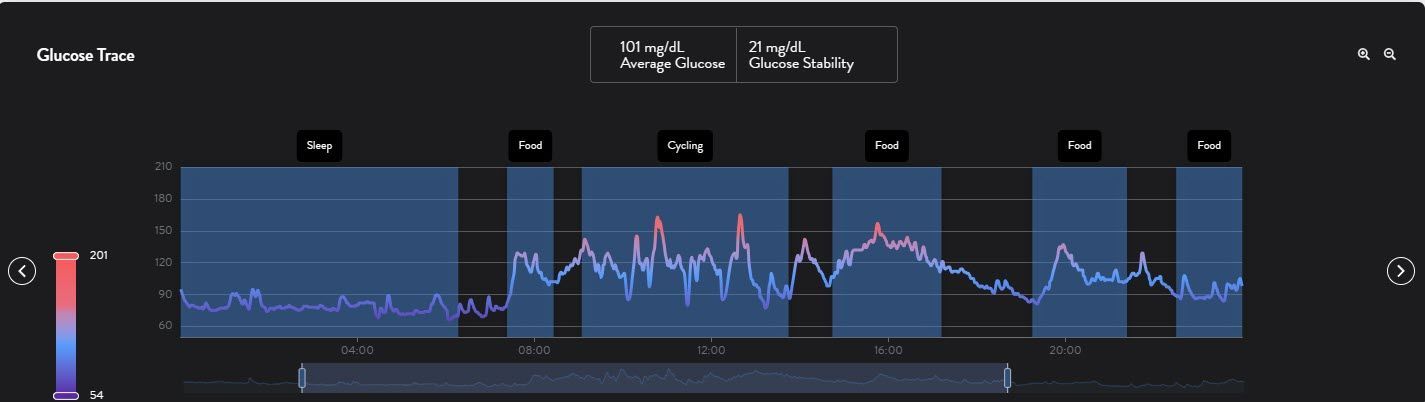
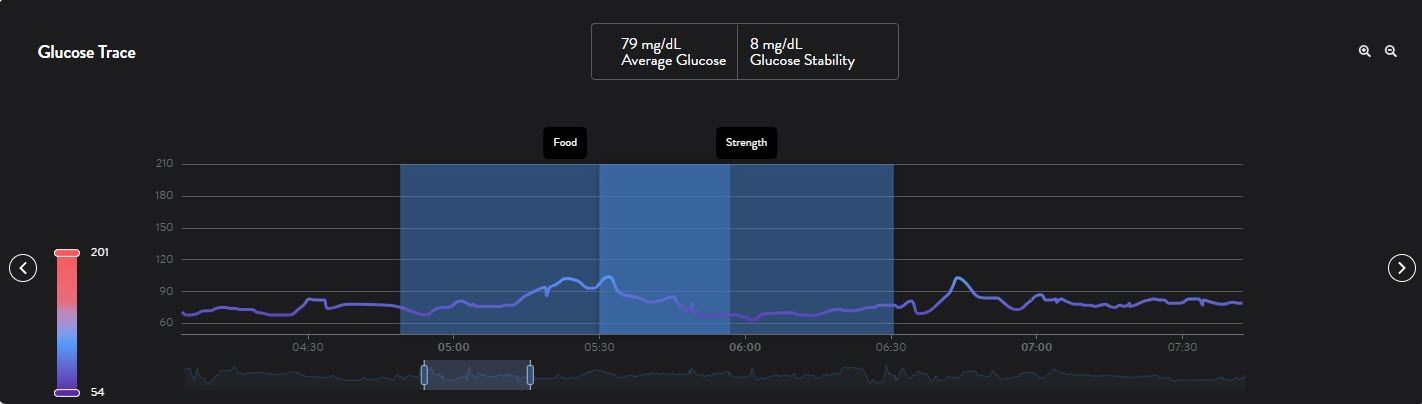
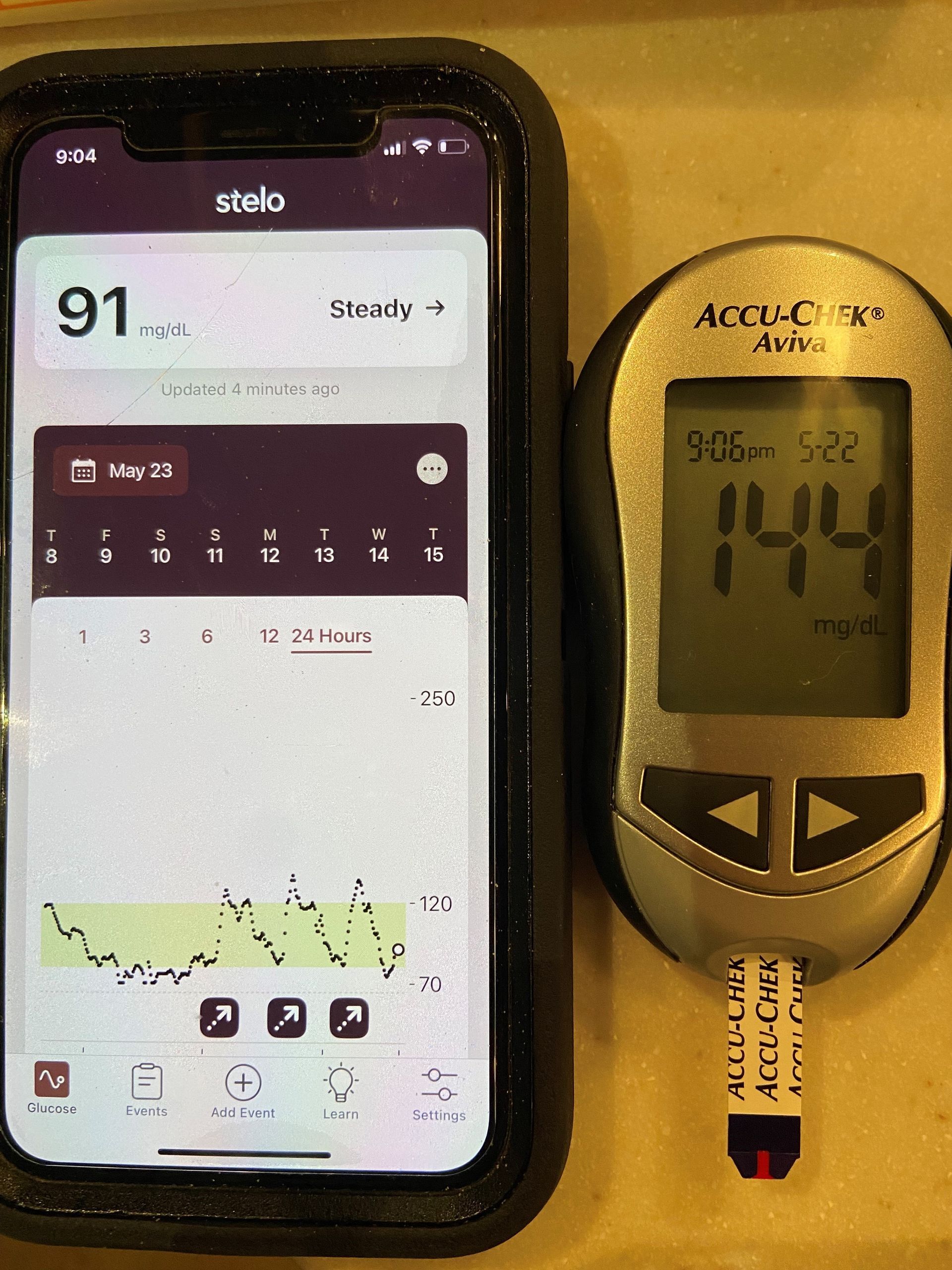
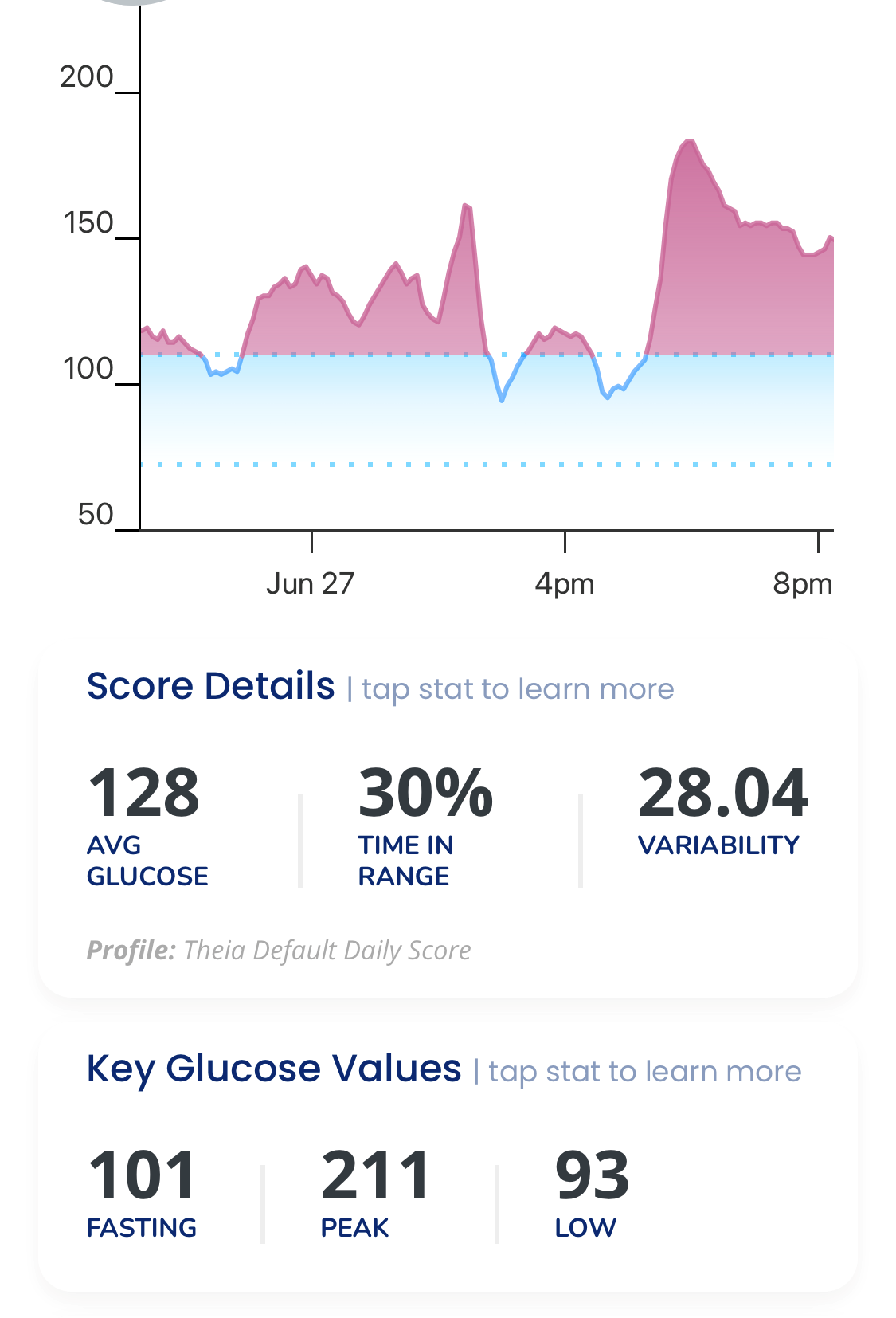
Real-world CGM data tells a similar story. Reviews of glucose patterns in endurance athletes show that average 24-hour glucose remains entirely normal, but athletes spend more time outside a narrow “textbook” range, with more frequent swings between mild hypoglycemia and exercise-induced hyperglycemia than sedentary individuals[6]. Rather than signaling dysfunction, this variability reflects a metabolism that is actively and rapidly reallocating fuel sources in response to training demands — precisely the glucose-sparing behavior at work. The researchers behind these reviews are explicit that standard non-athlete reference ranges and assumptions shouldn't be applied uncritically to trained endurance populations[6].
Why This Matters — and Why It's Not the Same as Diabetic Insulin Resistance
It's worth being precise about what distinguishes physiologic insulin resistance from the pathological insulin resistance associated with type 2 diabetes and metabolic syndrome, because the surface-level lab finding — a somewhat blunted glucose or insulin response — can look superficially similar.
First, context and reversibility: the athlete's pattern is a short-term, exercise-triggered shift tied to glycogen depletion and elevated fat oxidation, and it resolves within a day or two as glycogen stores are replenished[5]. Pathological insulin resistance is chronic, persists at rest, and worsens over time without intervention.
Second, tissue health: in physiologic insulin resistance, the muscle itself remains highly insulin-sensitive overall and metabolically efficient; the temporary glucose intolerance is a deliberate, adaptive prioritization of fuel, not a sign of impaired insulin signaling machinery[2,3]. In type 2 diabetes, insulin resistance reflects genuine impairment of insulin signaling, chronic low-grade inflammation, and ectopic fat accumulation in tissues that aren't built to handle it.
Third, the broader metabolic picture is opposite: endurance athletes as a group have outstanding cardiovascular fitness, favorable lipid profiles, and low visceral adiposity — the very risk factors that typically accompany pathological insulin resistance are largely absent[2,3,4]. Athletic training, including strategies like periodically training with lowered glycogen availability, actually enhances the body's capacity for this healthy fuel-switching and improves long-term metabolic flexibility[7,8].
Practical Takeaways for Athletes
If you see a temporarily elevated fasting glucose, a blunted CGM response, or an unimpressive oral glucose tolerance test result after a long ride, run, swim, or triathlon block, this is not necessarily cause for alarm — it may simply be your trained physiology doing exactly what it's supposed to do: sparing glucose for your brain and nervous system while your muscles run on fat. That said, individual variation exists, and any persistent or unexplained glucose abnormality — particularly outside the context of recent heavy training — deserves discussion with a physician or sports medicine specialist familiar with athlete physiology, since standard clinical assumptions don't always translate cleanly to a highly trained population[6].
Understanding this concept can also reduce unnecessary anxiety around glucose monitoring trends that have become popular among endurance athletes, and can inform smarter interpretation of lab work, recovery nutrition timing, and periodized fueling strategy — all built on the same underlying principle: your body isn't broken, it's adapted.
References
1. Randle PJ, Garland PB, Hales CN, Newsholme EA. The glucose fatty-acid cycle: its role in insulin sensitivity and the metabolic disturbances of diabetes mellitus. Lancet. 1963;281(7285):785-789.
2. Goodpaster BH, He J, Watkins S, Kelley DE. Skeletal muscle lipid content and insulin resistance: evidence for a paradox in endurance-trained athletes. J Clin Endocrinol Metab. 2001;86(12):5755-5761.
3. Amati F, Dubé JJ, Alvarez-Carnero E, et al. Skeletal muscle triglycerides, diacylglycerols, and ceramides in insulin resistance: another paradox in endurance-trained athletes? Diabetes. 2011;60(10):2588-2597.
4. Goodpaster BH, et al. Mechanistic insights into the exercise-induced changes in muscle lipids and insulin sensitivity—expanding on the “athlete's paradox”: revisiting a 2011 Diabetes classic by Amati et al. Diabetes. 2025;74(2):134.
5. Flockhart M, Tischer D, Nilsson LC, et al. Reduced glucose tolerance and insulin sensitivity after prolonged exercise in endurance athletes. Acta Physiol (Oxf). 2023;238(4):e13972.
6. Flockhart M, Larsen FJ. Continuous glucose monitoring in endurance athletes: interpretation and relevance of measurements for improving performance and health. Sports Med. 2024;54(2):247-255.
7. Van Proeyen K, Szlufcik K, Nielens H, Ramaekers M, Hespel P. Beneficial metabolic adaptations due to endurance exercise training in the fasted state. J Appl Physiol. 2011;110(1):236-245.
8. Jeukendrup AE. Carbohydrate dependence during prolonged, intense endurance exercise. Sports Med. 2015;45(Suppl 1):S91-S99.